
Potassium Iodide Pill Working Group Phase I Workshop Meeting Minutes
Date
November 4 and 5, 2019
Agenda
- Safety Brief
- Opening Remarks
- Introductions and an Overview of Workshop Objectives
- CANDU Design Features
- OPG Emergency Response Organization (ERO)
- Provincial Nuclear Emergency Response Plan (PNERP)
- OPG KI Pill Availability
- Distribution of KI in an emergency
- Municipal roles and responsibilities, communications, and plans
- Durham Region
- City of Toronto
- York Region
- City of Peterborough
- OPG Communications
- Safety Brief
- Municipal roles and responsibilities, communications, and plans (cont’d)
- Region of Peel
- City of Kawartha Lakes
- Simcoe Muskoka
- Health Canada’s Role in a Nuclear Emergency
- National and International Practices
- Tabletop Exercise
- Lessons learned and feedback on tabletop discussion/additional items
- Path forward for draft report
- Closing Remarks
Workshop Day 1 commenced at 09:00 on Monday November 4, 2019.
1. Safety Brief
OPG provided a safety brief to the Workshop participants. The safety brief covered procedures for responding to a medical emergency, fire emergency and station emergency.
2. Opening Remarks
The Signatories of the Potassium Iodide (KI) Pill Working Group provided opening remarks and welcomed participants to the KI Pill Working Group Phase I Workshop.
The Signatories reiterated that the purpose of this workshop is to provide an opportunity for all Working Group members to work collaboratively on fulfilling the deliverables set out for Phase I as per the Terms of the Reference (TOR).
3. Introductions and an Overview of Workshop Objectives
There was a roundtable introduction of workshop participants. The following organizations were represented:
- Signatories to the TOR: CNSC, the Office of the Fire Marshal and Emergency Management (OFMEM), the Ontario Ministry of Health (MOH) and Ontario Power Generation (OPG)
- Public Health Units (PHUs) from Peel Region, York Region, City of Toronto, Durham Region, Simcoe Muskoka District, Haliburton-Kawartha-Pine Ridge District, and Peterborough
- Community Emergency Management Coordinators (CEMCs) from Durham Region, the Region of Peel, Regional Municipality of York, City of Kawartha Lakes, City of Peterborough and the City of Markham.
- Other: Health Canada and the Public Health Agency of Canada (PHAC)
CNSC reiterated that the primary objective of the Working Group was to provide clarity on roles and responsibilities for KI pill distribution during an emergency within the 50 km Ingestion Planning Zone (IPZ) of the Pickering Nuclear Generating Station (NGS).
Specifically, the information presented during the workshop is intended to cover the strategy for Phase I of the Working Group and focussed on the following items:
- Current provincial and federal requirements for the distribution of KI pills;
- Considerations and education concerning KI pill emergency distribution in the IPZ;
- Means of KI pill distribution in relation to other factors associated with a nuclear emergency response; and,
- Availability and scope of public emergency preparedness information related to KI pills.
Following the workshop, a draft copy of the meeting minutes would be available to the Working Group members for review within 10 business days. Members will then have an additional 10 business days to provide comments so that the minutes can be prepared for approval. Meeting minutes of the workshop will be made publicly available on the CNSC website in French and English following concurrence of the minutes by all Working Group members.
4. CANDU Design Features
This item was included in the workshop to provide more context of CANDU Nuclear Power Plants (NPPs) for workshop participants who do not have a strong technical background in this area.
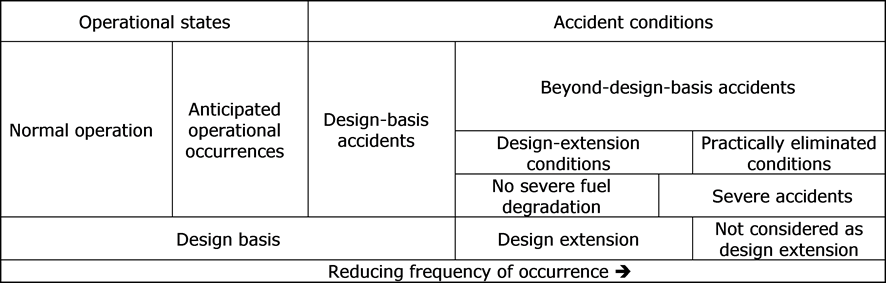
OPG provided a brief background of Design Basis Accidents (DBAs) and Beyond Design Basis Accidents (BDBAs), and the defence-in-depth in place to manage such accidents. OPG referenced the CNSC Regulatory Document REGDOC-2.4.1, Deterministic Safety Analysis to show the range of plant states as it relates to DBAs, BDBAs, and their frequency of occurrence (Figure 1). It was emphasized that DBAs have a very low probability of occurring with a frequency of occurrence equal to or greater than 10-5 per reactor year, but less than 10-2 per reactor year. BDBAs have an even lower probability of occurring with a frequency of occurrence less than 10-5 per reactor year.
Text version
Figure 1 shows the different plant states, illustrating how they are considered in the design of a nuclear power plant. It is structured like a table.
First Row
Reading left to right, the first row contains two boxes labelled "Operational states" "Accident conditions"
Second Row
Under the "Operational states" box are two boxes labelled "Normal Operation" and "Anticipated operational occurrences".
Under the "Accident conditions" box are two boxes labelled "Design-basis accidents" and "Beyond-design-basis accidents".
Third Row
Under "Beyond-design-basis accidents" box are boxes labelled "Design-extension conditions" and "Practically eliminated conditions".
Fourth
Under the "Design-extension conditions" box is a box labelled "No severe fuel degradation" and a portion of a box labelled "Severe accidents".
Under the "Practically eliminated conditions" box is a box labelled "Severe accidents".
Fifth Row
Reading left to right:
Under the boxes "Normal operation", "Anticipated operational occurrences" and "Design-basis accidents" is a box labelled "Design basis".
Under the "No severe fuel degradation" box is a box labelled "Design extension".
Under the "Severe accidents" box is a box labelled "Not considered as design extension"
Sixth Row
At the base of the table is a box labelled "Reducing frequency of occurrence" with an arrow pointing to the right. Reading left to right, the boxes of the table are presented in order of reducing frequency of occurrence: "Normal operation", "Anticipated operational occurrences", "Design-basis accidents" and "Beyond-design-basis accidents".
For DBAs, OPG described the range of accident categories, the materials that could be released from the core to containment (e.g. noble gases, vapours, and aerosols), and the special safety systems available to mitigate accident consequences. In all DBAs, the NPPs are designed to filter 99.5% of contaminants, protecting the public and the environment. In BDBA, filtered venting would also be utilized to the extent possible.
OPG also highlighted the differences between a DBA and a BDBA, and explained the additional barriers in place to manage BDBAs (e.g. emergency mitigating equipment (EME)). OPG emphasized that lessons learned from events such as the Fukushima Daiichi accidents have been used to strengthen defence-in-depth for all Canadian NPPs.
Discussion items:
- Accident progression timeline: Participants inquired about the timeline associated with accident progression, specifically the timings of a release for a BDBA. OPG indicated that when an event goes into a BDBA, it could take approximately 20+ hours prior to the first release in the very unlikely event that all safety systems failed. For a more likely, but still very unlikely DBA, the minimum time before a release is 47 hours for Pickering NGS. Updates are provided regularly to the Province and the CNSC should this timing change during an emergency. Participants considered this a very important piece of information as this gives a perspective for the timings associated with decision-making and implementing protective actions.
- Transition from DBA and BDBA: A participant inquired about when a DBA transitions to a BDBA, and the factors considered in making that determination. OPG indicated that many factors are considered to make that determination, and indicated that plant parameters and safety systems are continuously being monitored to understand how the event is progressing. Any updates on of the plant status and progression are continuously provided to the CNSC, the Province, and other external stakeholders.
- BDBA initiating event: Participants sought confirmation on whether it was appropriate to say that a DBA would be initiated by an internal hazard within the station, and a BDBA would be initiated by an external hazard. OPG agreed to an extent but emphasized that it is more dependent on the status of the barriers in place to manage the event. As an example, OPG indicated that an event caused by an external hazard in which the safety systems are available would be considered a DBA. In comparison, an external hazard of significant magnitude resulting in the loss of power and unavailability of safety systems would be considered a BDBA.
- CANDU events: Participants inquired about whether there have been any CANDU events resulting in uncontrolled releases. OPG indicated that any known releases were not a result of an event, and did not exceed any regulatory release limits.
5. OPG Emergency Response Organization (ERO)
OPG provided an overview of the OPG Emergency Response to an event and provided information on:
- Event classification and incident categorization.
- Requirements and timelines for sending notifications to the province, the CNSC, and other external stakeholders. It was noted that upon event classification and categorization, the province would be notified within 15 minutes via verbal confirmation and a notification form through fax and/or OPG WebEOC.
- Event categories defined in the Provincial Nuclear Emergency Response Plan (PNERP): Reportable event, abnormal incident, onsite emergency, and general emergency.
- Plant parameter data transmitted to the province and the CNSC on an hourly basis.
- Onsite/Offsite survey data provided to offsite agencies.
- OPG liaison staff dispatched to offsite organizations (e.g. provincial and municipal emergency operations centres).
6. Provincial Nuclear Emergency Response Plan (PNERP)
OFMEM and MOH provided an overview of provincial nuclear emergency management, emergency planning zones, protective measures, concept of operations, and iodine thyroid blocking.
-
Provincial Nuclear Emergency Management
OFMEM provided the legislative context for the PNERP under the Emergency Management and Civil Protection Act (EMPCA), and the role of the province of Ontario as it relates to managing offsite consequences and response.
The PNERP details the response to nuclear and radiological emergencies, which could affect the health, safety and welfare of the people of Ontario, and the protection of property and the environment.
The PNERP – Master Plan (2017) provides the overall policies, organization and processes for responding to a nuclear emergency. Subsequent to the Master Plan are the site specific implementing plans (IP); the specific plan for Pickering was approved in 2019.
-
Emergency Planning Zones
The four planning zones as defined in the PNERP are the 3 km Automatic Action Zone (AAZ), 10 km Detailed Planning Zone (DPZ), 20 km Contingency Planning Zone (CPZ), and 50 km Ingestion Planning Zone (IPZ). Emphasis was put on the CPZ as it was recently added in the PNERP in 2017 to facilitate response (e.g. public alerting, iodine thyroid blocking (ITB), and public awareness and education) for extremely low probability events.
Note: Unless otherwise specified, references to the IPZ in this document include the CPZ.
-
Protective Measures
OFMEM explained that there are two categories of protective measures: (1) exposure control measures to protect against direct exposure and inhalation of radioactive particulates and (2) ingestion control measures to protect against indirect exposure to radiation. It was noted that exposure control measures (i.e. shelter in place, evacuation, KI pill ingestion) would normally be limited to the DPZ, and ingestion control measures (i.e. food restrictions) would normally be implemented in the IPZ.
It was noted that ITB (i.e. KI pills) provides protection against one radioisotope (Iodine – 131) and would normally be implemented in combination with another exposure control measure such as evacuation or sheltering-in-place in order to limit exposure from all radioisotopes.
-
Concept of Operations
OFMEM explained the concept of operations for the activation of the Provincial Emergency Operations Centre (PEOC). Information was provided on how the PEOC would be notified by the licensee, and how notifications would be sent out and received by the municipalities. Based on the event, the PEOC will then determine whether their EOC needs to be activated, and the type of analysis that should be done to begin planning for protective actions if required.
OFMEM indicated that a provincial response from a DBA to a BDBA would differentiate due to the timing of the event progression. As an example, a DBA would have a longer hold-up time of materials within containment allowing more time for filtering to occur, and to determine the appropriate protective actions. In any case, however, the PEOC Scientific Section would be activated to undertake analysis and determine which protective actions are required.
A protective action recommendation to take ITB would be directed by the Ontario Chief Medical Officer of Health (CMOH) in coordination with the PEOC and the local Medical Officer(s) of Health.
-
Iodine Thyroid Blocking (ITB)
MOH presented background information on the use of KI in an emergency and the information provided in the MOH Radiation Health Response Plan (RHRP) (2014) and the subsequent MOH Potassium Iodide Guidelines (2014). These plans provide guidance and coordination for stocking, distribution, and administration of KI, and defines the vulnerable population as pregnant and breast feeding women, infants, and children under 18 years of age.
Discussion items:
-
Updating plans: Participants inquired about whether there are any plans in place to update the MOH RHRP and the KI Guidelines to align with the 2017 PNERP. MOH indicated that there are no plans in place to update these documents; however highlighted that aside from some terminology, the information is still relevant.
-
Availability of KI pills: Participants inquired about whether a situation can be foreseen where there is mass fear on not knowing where to get KI or from people beyond the IPZ requesting KI pills during an event. Some municipalities shared what they have in place, for example, Durham Region indicated that limited quantities are available at three Pickering pharmacies. Durham Region manages the majority of requests through the www.preparetobesafe.ca website.
-
Evacuation strategy: Participants inquired about how long it would take to evacuate the DPZ for Pickering. OFMEM indicated that there are many factors to consider and it could take 8 – 9 hours; participants were encouraged to look at the evacuation study that was posted to the OPG website.
It was discussed that the Ministry of Transportation (MTO) works with the local police, roads departments, and CEMCs of the designated and surrounding municipalities to develop a traffic management plan for evacuation. Participants inquired about whether this plan considers those who cannot evacuate on their own. Municipalities provided some insight, but indicated that only limited planning data is available. Beyond the nuclear issue, some municipalities consider other factors related to moving people out and would coordinate with organizations such as the provincial joint Traffic Control Centre.
7. OPG KI Pill Availability
OPG presented on the availability of KI pills in the DPZ and IPZ, and discussed the campaigns in place to enhance public awareness and education, and maintain KI pill inventories.
In January 2015, OPG developed a two-part public awareness campaign. The first part was the pre-distribution campaign that focussed on education to raise public awareness of KI distribution targeted to the residences and businesses within the DPZ. The second part was the distribution campaign that utilized product packaging to improve the public’s understanding of when and how to use the KI pills. Both campaigns use the OPG www.preparetobesafe.ca website as an official online source of information for KI pills and emergency preparedness, as well as for residents in the IPZ to order KI pills that are delivered, free of charge.
-
Distribution to DPZ
Since 2015, there is a focus on the KI pre-distribution sustainability to ensure that any new residences and businesses within the DPZ receive a package of KI pills. This is done through the New Neighbours Program that uses data from Canada Post to identify any address changes. To date, there have been approximately 1.7 million KI pills distributed through this program for the Pickering and Darlington DPZs. Expired KI for institutions and first responders was replenished within Durham region in 2019.
-
Distribution to IPZ
Residences and businesses within the IPZ of Pickering and Darlington can order a supply of KI pills through the preparetobesafe.ca website. To date, there have been approximately 700,000 KI pills distributed through the preparetobesafe.ca website for the Pickering and Darlington IPZs. Expired KI for first responders was replenished within Durham region in 2019.
-
Distribution to emergency response facilities
At the Emergency Workers Centres (EWCs) and Mobile Monitoring and Decontamination Units (MMDUs) there are approximately 11, 500 KI pills available. Reception Centres (RCs) have approximately 27,000 KI pills available at each centre.
Prior to 2015, OPG in coordination with other stakeholders had pre-distributed KI pills to first responders and institutions that had an expiration date of April 2019. In early 2019, this inventory was replenished with a new inventory with an expiration date of 2029.
Discussion items:
-
KI pills metrics: Participants inquired about the metrics that are available for KI pill distribution. Specifically, metrics relating to the exact locations for where they were distributed, returned products/inventories, and information on the individual requests from preparetobesafe.ca. OPG noted that personal information could not be released however; it is possible to get metrics from the website for the number of pills within a given area based on postal codes.
8. Distribution of KI in an emergency
MOH presented the current KI pill distribution strategy as it relates to the preparedness and response phase of emergency management.
-
Preparedness
As presented by OPG, KI pills are currently pre-distributed to all residences and business within the 10 km DPZ, and available to anyone within the 50 km IPZ by request at preparetobesafe.ca.
-
Response
The decision to administer KI is made by the Chief Medical Officer of Health (CMOH) in consideration of input from the local Medical Officers of Health and the Scientific Section of the PEOC. It was reiterated that the ingestion of KI would always occur in conjunction with other protective measures, such as evacuation or shelter-in-place.
A stockpile of 6 million pills is held at a warehouse facility in the Toronto area on behalf of OPG. This facility can be accessed 24/7 and has a sufficient stockpile of KI pills for the whole IPZ population. Emergency distribution would be facilitated through the PEOC to local PHUs.
More operationally, if emergency distribution and ingestion of KI were ordered by the CMOH, the following actions would be taken: MOH to provide contact/access to the warehouse facility and delivery of KI pills to municipal authorities for further distribution/pick-up for locations deemed appropriate.
Discussion items:
-
Roles and responsibilities for pick-up and distribution: It was clarified that pick-up from the warehouse would be done by the province and delivered to the municipalities. Participants wanted further clarification on whether municipalities means the PHUs, the CEMCs, or both. It was noted that some municipalities do not have overarching PHUs, instead the PHUs are linked to the lower tier municipalities; therefore, it was unclear how notification and coordination between the province and the municipality is conducted. MOH confirmed that they would liaise with the PHUs to provide notifications and relay any updates from the province. There was a request for clarification from PHUs regarding the administration of KI. Administration strategies, such as information and self-administration, will be considered as part of Phase II of the Working Group.
-
Distribution timing: Participants inquired about how long it would take the distribution to take place. OFMEM indicated there are many things that would need to be considered, and a study to that level of detail has not been conducted. Phase II of this Working Group is intended to focus on the feasibility of these plans and will help inform those details.
Participants inquired about whether it is expected that CEMCs would send staff into “hot zones” to distribute KI pills. OFMEM confirmed that the ingestion of KI pills would take place prior to the plume passing, and therefore sending staff into a plume to distribute KI pills would not occur. MOH also confirmed that the order to take KI pills would be communicated to the public through emergency bulletins and communications well in advance, if a release were to occur.
-
Pre-staged stockpiles: Participants inquired about whether there were transportation issues that would hinder moving the stockpile during an emergency. OFMEM and MOH indicated that they were considering redistributing the warehouse supply to a number of strategically located facilities that may facilitate more rapid distribution at the start of an emergency, prior to an emission.
It was noted that these stockpiles would be located across the IPZ, however distribution would still be dependent on the meteorological conditions and the potential areas affected. Participants noted that even though it would be dependent on where the plume is moving, populations across the IPZ will still be looking for KI pills. OFMEM noted this is where public education is so important to make sure the ingestion of KI pills is understood by the public. This needs to be a priority when discussing these arrangements.
Participants inquired why KI pills could not be pre-distributed within the IPZ since there are already enough pills. OFMEM reiterated that based on the planning basis of the PNERP, the entire IPZ would not be required to take KI pills in the unlikely event of a nuclear emergency. Implementation would be focussed on specific areas known as keyholes. It was reiterated that this is where public education is important. In addition, this level of contingency comes with many logistical constraints and effort given the population density of the 50 km IPZ around the Pickering station.
-
Planning zones: Participants inquired about why the IPZ would require KI pill ingestion in the first place, given that the IPZ is intended to protect against indirect exposure. OFMEM firstly indicated that the planning zones are planned around evacuation not KI pills ingestion. MOH then reiterated that the ingestion of KI pills in the IPZ would only be required in an extremely unlikely accident scenario.
Participants inquired about why the planning would not be around an extremely unlikely accident scenario. OFMEM explained that the frequency of such an event would be extremely low and in emergency management, it is difficult to have detailed plans to that extent. For KI pills distribution it is more appropriate to have a program/strategy in place rather than a detailed plan. Again, it was reiterated that public education, as well as communications for KI Pill distribution during an emergency is important.
-
Evacuation: Participants inquired about whether evacuees from the IPZ would be instructed to take KI pills. It was confirmed that if populations were evacuated then they would be moving away from the direction of the plume and would not require ingestion of KI pills. Where evacuation may not be feasible in a timely manner, such as hospitals and old age homes, individuals and staff members at these facilities would be targeted for KI distribution.
Participants inquired about whether people evacuating would be contaminated with radiation and if this contamination could spread. OFMEM confirmed that populations would be evacuated prior to a release and therefore would not be contaminated, and there would be MMDUs in place to monitor evacuees if required.
-
Public awareness and communication: Participants heavily emphasised the importance of public education, awareness, and communications during emergency preparedness and response. Given the number of municipalities and stakeholders involved, it is imperative that the messaging is coordinated, consistent and provides the appropriate reassurance to the public.
9. Municipal roles and responsibilities, communications, and plans
In this section, various plans and policies not created for KI distribution are mentioned as possibly useful. These plans, as they are not intended for KI distribution, may or may not be utilized depending on the situation and other external factors.
The Durham Region and City of Toronto are identified as designated municipalities under the Pickering PNERP IP, and are required to have KI pre-distributed within the 10 km DPZ of the Pickering NGS. The two designated municipalities work closely with OPG and OFMEM to leverage communication products and campaigns to ensure consistent and coordinated messaging.
The City of Peterborough is beyond the 50 km IPZ and is identified as a host municipality under the Pickering PNERP Implementing Plan.
York Region, Peel Region, City of Kawartha Lakes and Simcoe Muskoka are within the 50 km IPZ for the Pickering NGS. These municipalities are not identified as a designated municipality and do not require pre-distribution of KI pills.
During an event response, all municipalities would look to OFMEM and MOH to initiate a notification to the municipalities and issue operational directives regarding implementation of protective measures.
Public communication and awareness strategies within the IPZ and in the City of Peterborough may involve leveraging preparetobesafe.ca in their communication products and reinforcing information released by OPG, OFMEM and MOH to ensure consistent messaging between the various levels of response during an emergency. Additional communication channels from each municipality (e.g. social media, media briefings, news releases, public inquiry lines, Alert Ready, etc.) would be used to ensure communications are being disseminated to the public in their region during an emergency. During the workshop, the municipalities’ representatives noted areas in which additional guidance would be helpful to enhance awareness and communications to the public.
9.1. Durham Region
-
Concept of Operations
The municipality works closely with OPG to promote their KI pill public awareness campaign, and holds a seat in the Ontario Nuclear Emergency Management Coordinating Committee (NEMCC). Durham Region also established the Durham Nuclear Health Committee (DNHC). This committee is a scientific and technical oriented committee focussed on nuclear emission, nuclear wastes and other related topics, and can be used as a public forum to address specific issues and concerns related to radiological emissions.
-
KI Pill Distribution
Durham Region Health Department recently redistributed new KI pills to all institutions within the DPZ, as well as to first responders with an expiry date of 2029. This was done in coordination with schools, private school, hospitals, long-term care facilities, municipal fire departments, Durham Regional Police, Region of Durham Paramedic Services, and youth detention centres. There is also a small quantity of KI pills available at select locations across Durham region such as local pharmacies.
Discussion items:
-
Awareness Campaigns: Participants inquired about whether Durham Region has identified aspects of campaigns that were deemed most effective (e.g. social media, advertisements, YouTube, etc.). The Durham Region representatives indicated that they do not track those metrics; however noted a decrease in social media inquires with the increase of public education and awareness.
-
First Responders: Participants inquired about whether First Responders have asked about needing additional information or materials. The Durham Region representatives indicated they work closely with the First Responders to ensure they are provided with information on KI pills, and are provided with copies of the MOH fact sheet and KI Guidelines.
9.2. City of Toronto
-
Concept of Operations
The municipality will activate the EOC to advise and coordinate with stakeholders. This includes but is not limited to the Toronto Police Service, Emergency Medical Services, Transportation Services, and Strategic Communications. The municipality would also ensure reception-evacuee centres and emergency worker centres are readied to become operational without undue delay.
-
KI Pill Distribution to the IPZ during an emergency
The City of Toronto may leverage existing plans such as the Toronto Public Health – Mass Immunization Clinic (MIC) Plan for implementation and staffing models.
9.3. York Region
-
Concept of Operations
During an emergency response, York Region CEMCs would utilize the Regional all-hazards emergency plan. The PHUs would fulfill their role under the MOH RHRP to support risk communications and public awareness, distribution of KI pills under the direction of the CMOH, and assessment of water and food safety.
-
KI Pill Distribution to the IPZ during an emergency
York Region maintains metrics for schools, childcare centres, pharmacies/drug stores, and households, which may be leveraged to identify publicly accessible areas should they have to distribute KI pills within their municipality. This information is collected for a different purpose and is protected under the Personal Health Information Protection Act (PHIPA), thus informed consent and other legal concerns must be addressed before it can be used in this way. It was noted however that if it were possible, it would be most efficient to have KI pills pre-distributed in or pre-positioned to the York Region population prior to an emergency.
9.4. City of Peterborough
-
Concept of Operations
The Peterborough Nuclear Emergency Response Plan conforms to the PNERP and details arrangements such as receiving and accommodating evacuees, coordination of reception centres plans with OPG’s monitoring and decontamination arrangements, and liaison arrangements with designated municipalities and the PEOC. They work closely with strategic partners such as Fleming College (designated reception centre) and emergency responders, and regularly conduct drills and exercises in coordination with OPG.
-
KI Pill Distribution to the IPZ during an emergency
The Peterborough reception centre has KI pills available. It was noted that more messaging and resources for ingesting KI pills would be beneficial at the reception and evacuation centres should there be inquiries during an event.
Discussion items:
- Evacuation Centres: Participants inquired about the capacity of the Peterborough evacuation centres. The City of Peterborough representative indicated that this could vary depending on the time of year, the resources available and the time allotted to free up resources. For example, the University/College Residences could be used during the summer when there are less students, but may not be readily available during the school year.
10. OPG Communications
OPG provided insights to some of the communication tactics used to communicate with the public on KI pills. Some tactics include:
- Face-to-face opportunities such as public information centres, open houses and community information sessions, OPG programs and events, annual Council briefings, community advisory council meetings, and attending meetings for the Durham’s Nuclear Health Committee.
- Direct mail and print: quarterly newsletter (to 200,000 homes), local recreation guides and magazines, and brochures and KI pill packages in collaboration with the province, Durham Region, and City of Toronto.
- OPG.com provides information that is relevant, easy to find and easy to understand.
- Social media: geo-targeted twitter and Facebook safety campaigns, share Durham Emergency Management communications on public alerting testing, and share Durham Public Health communications on KI pills.
OPG engages directly with the public through community safety surveys, and tracking inquiries and interventions to help craft key messages and communications effectiveness. With respect to KI pill distribution specifically, OPG found that 86% of those were who surveyed indicated that they were aware of the KI pill campaigns, and recalled receiving KI pills from OPG.
Discussion items
- Municipality collaboration: Participants inquired about whether OPG works directly with other municipalities beyond Durham Region and Toronto as it relates to communications. OPG indicated that the focus is on the designated municipalities with pre-distributed KI pills. However, OPG provides support through preparetobesafe.ca to those municipalities beyond the 10 km DPZ.
Workshop Day 1 ended at 16:00 on Monday November 4, 2019.
Workshop Day 2 commenced at 09:00 on Tuesday November 5, 2019.
11. Safety Brief
OPG provided a safety brief to the workshop participants. The safety brief procedures for responding to a medical emergency, fire emergency and station emergency.
12. Municipal roles and responsibilities, communications, and plans (cont’d)
12.1. Region of Peel
-
Concept of Operations
In the event of an emergency, the Regional Emergency Management (REM) would coordinate response activities with the PEOC, local and neighbouring municipalities, and internal and external stakeholders. The Peel PHU would support provincial and REM activities and provide information to health practitioners and the public.
-
KI Pill Distribution to the IPZ during an emergency
The Region of Peel would leverage existing plans for KI pill distribution such as the vaccine distribution plan through multi-service clinics and evacuation plans. Distribution to local pharmacies could also be considered.
12.2. City of Kawartha Lakes
-
KI Pill Distribution to the IPZ during an emergency
During an emergency, the City of Kawartha Lakes will continue to reinforce and disseminate communications from OPG, OFMEM and MOH for taking KI pills. Pre-distribution of KI pills would occur for staff working in the IPZ. The CEMCs would coordinate with the Haliburton Kawartha Pine Ridge District Health Unit on the locations of evacuation centres and/or distribution centres requiring KI pills.
-
Concept of Operations
In the event of an emergency, the City of Kawartha Lakes Emergency Management would activate the emergency plan in place for all hazards if required. Activities and communications would be coordinated with the PEOC, local and neighbouring municipalities and stakeholders as necessary. Emergency Management would coordinate with the Haliburton Kawartha Pine Ridge District Health Unit in the event of a health emergency for dissemination of public health information with assistance from the City of Kawartha Lakes Communications team.
12.3. Simcoe Muskoka
-
Concept of Operations
Simcoe Muskoka would leverage plans in place for all-hazards emergency planning, and chemical, biological, radiological, nuclear and explosive (CBRNE) events for responding to an event at the Pickering NGS. Some of their roles and responsibilities under these plans include providing direction/advice to appropriate agencies/public related to the health hazards or health effects, providing active/passive surveillance for those exposed and released from the event “site”, and supporting in coordination efforts at evacuation shelters.
-
KI Pill Distribution to the IPZ during an emergency
During an emergency, Simcoe Muskoka can leverage existing plans such as reception centre and evacuation shelter management plans (e.g. County of Simcoe Evacuation Shelter Operational Plan), and mass immunization plans to conduct distribution of KI pills.
13. Health Canada’s Role in a Nuclear Emergency
Health Canada (HC) provided an overview of HC’s Role in a nuclear emergency at the OPG Pickering NGS. Specifically, HC presented the Federal Emergency Response Plan (FERP) and the Federal Nuclear Emergency Plan (FNEP). The FERP is the Government of Canada’s “all-hazards” response plan, led by Public Safety Canada, and the FNEP is an event-specific annex to the FERP, led by HC. Within the FNEP, is the Ontario Annex, which serves as the pre-arranged agreements between the federal and provincial governments, regarding assistance during a nuclear emergency.
During the preparedness phase, HC provides guidance, advice, and technical support in the areas of generic criteria (including criteria for stable iodine thyroid blocking), operational intervention levels, and dispersion and dose modelling for nuclear emergency planning and response.
During the response phase, the FNEP Technical Assessment Group (TAG) will be stood-up to provide technical support to responding agencies. Among other areas of the technical support, the FNEP TAG Situational Awareness and Risk Assessment Group would collect and analyse information, including dispersion and dose modelling, and communicate the results to appropriate authorities. The FNEP TAG Support to Communications Group would execute the communication strategy – by ensuring coordination of communications across federal and provincial departments and agencies and supporting the Chief Public Health Officer (CPHO) as the federal spokesperson.
HC also provided information on the Public Health Agency of Canada National Emergency Strategic Stockpile (NESS). The NESS contains supplies that provinces and territories can request in emergencies when their own resources are not sufficient. NESS also contains a small supply of KI pills intended for federal employees such as field monitoring teams. In general, supplies are stored in a central depot in the National Capital Region and in warehouses strategically located across Canada.
14. National and International Practices
CNSC presented on national and international practices for distribution of KI pills. The national practices considered the CNSC regulatory requirements for distribution of KI pills, and the plans in place for the Bruce Nuclear Generating Station, the Point Lepreau Nuclear Generating Station, and for the Windsor and Essex County residing in then planning zones for the US Enrico Fermi 2 Nuclear Generating Station.
The international practices included distribution of KI pills in countries such as France, Switzerland, United Kingdom, Finland and the United States. Internationally, it was noted that the plans in place were dependent on governing legislation, NPP designs, and population densities, and thus there were variations in the distribution mechanisms. For example, in France, distribution campaigns are used to send coupons and information to residents and directors of businesses and public institutions in the 10 km zone of a nuclear power plant that can be redeemed for KI pills. In comparison, Switzerland, under the direction of their Federal Council in 2014, KI pills were pre-distributed to all residents and businesses within 50 km of each plant.
Discussion items:
-
Bruce Power: Participants inquired about whether KI pills have been distributed to the schools within the Bruce Power 50 km IPZ for administering KI pills to students or for activating as a reception centre for the populations in the surrounding areas.
Action: CNSC to follow-up on the purpose for Bruce Power pre-distributing to schools within their IPZ.
-
New Brunswick Power: Participants inquired about whether First Responders in New Brunswick were pre-distributed with KI pills.
Action: CNSC to follow-up on whether first responders in New Brunswick were pre-distributed with KI pills.
-
OPG: Participants inquired about how members of the public who work within the Pickering IPZ can request KI pills. OPG confirmed that the preparetobesafe.ca website allows workers within the IPZ to input their work address to request KI pills.
-
REGDOC 2.10.1: The CNSC regulatory requirements state that: residents of the designated ingestion control planning zone can obtain KI pills at any time. Participants questioned why businesses and institutions were not included. OPG and OFMEM confirmed that it was included in their plans regardless.
-
US Planning Zones: Participants inquired about why the Fermi planning zone is 80 km and Ontario’s is 50 km. It was confirmed that the 80 km is based on the US NRC and FEMA requirements, and is dependent on the NPP designs and the planning basis for the plants in the US.
-
KI Pills Vouchers: Participants inquired whether it should be left to the public to make an educated decision based on information and resources provided to determine if they would like KI pills or not. It was noted that the uptake on using the vouchers in the US was very low.
-
Public Communications: Participants highlighted the importance of having a risk communication mechanism to understand things such as the differences between US planning zones vs. Canadian planning zones. Participants also raised concerns that KI pills are being portrayed as “anti-radiation” pills, and believe there needs to be more messaging to the public to dispute this claim.
15. Tabletop Exercise
The tabletop exercise was intended as an open discussion to consider the factors involved in facilitating KI distribution during an emergency at the Pickering NGS. The following relates to the tabletop exercise within the context of KI distribution and does not represent the full scope of emergency response for a nuclear emergency. Each stakeholder was given the opportunity to explain their roles and responsibilities, and elaborate on the coordination between other stakeholders as it relates to emergency response actions within the Pickering IPZ. It was noted that onsite conditions and actions are out of scope for this exercise. It was also noted that KI pills only prevent radioactive Iodine-131 from accumulating in the thyroid, are not anti-radiation pills, and do not protect against any other radioactive substances or external radiation (i.e. radioactivity deposited in the environment/surfaces, or on foods).
-
Event Notifications (e.g. reportable event)
OPG Notifications: OPG is required to notify the province (e.g. PEOC) and Designated Municipalities within 15 minutes of initial categorization of an event at the Pickering NGS and the CNSC within 15 minutes of Emergency Response Organization (ERO) activation. The province, Designated Municipalities, and the CNSC would also be notified of any changes to the event categorization. Notification would be received via verbal confirmation and the transmittal of an OPG notification form.
Provincial/Municipal Notifications: The event categorization will determine which stakeholders the province will notify. For notification categories above Reportable Event, the PEOC will notify all stakeholders including the designated municipalities (i.e. Durham Region and the City of Toronto), who must be notified within 15 minutes, of the Provincial Response Level. The MOH will follow up this notification with its own pre-established communications to relay this notification to municipal PHUs. Upper-tier municipalities (PHUs/CEMCs) would notify lower tier municipalities, according to their notification protocols.
Federal Response: Similarly, depending on the event categorization, the CNSC may send event notifications to Federal partners such as Health Canada, and the International Atomic Energy Agency (IAEA).
Public Communications: For a reportable event, there would be no information released to the public given there is no offsite safety concerns. In any case, communication teams may begin monitoring social media and news releases upon initial notification to address any public inquiries that may arise.
-
Event Re-categorization (e.g. Reportable event upgraded to Onsite Emergency)
OPG Activation: Assuming that an event is upgraded from a reportable event to an onsite emergency, OPG would have activated the onsite ERO and would begin sending hourly updates to OFMEM and the CNSC. OPG may also begin standing up off-site emergency centres to ensure prompt activation if/when required.
Provincial Activation: At this point, the province will adopt a partial activation response (Activation levels are defined in Section 5.5 of the PNERP - Master Plan) which involves the full staffing of the PEOC with the Scientific Section monitoring plant conditions and assessing event progression, through the hourly updates received from OPG. The PEOC will include liaison staff from various organizations at the federal, provincial and municipal levels, and incident briefings will be issued to relevant stakeholders. At this point, it is assumed that no protective actions are required.
Municipal Activation: MOH will continue to liaise pertinent information to the Public Health Care Providers. Upon activation of MOH, logistical arrangements for sheltering and evacuating planning would have began. Designated Municipalities may have partially activated their EOCs, and the CEMCs and PHUs would begin liaising information between each other. For the other municipalities within the IPZ (York, Peel, Simcoe and Kawartha Lakes), they may be at Enhanced Monitoring until further information is provided.
Federal Activation: CNSC would upgrade their activation level depending on the event progression. For Partial and Full Activation, the CNSC and the province would have notified the Health Canada FNEP Duty Officer who would then activate the FNEP. The FNEP TAG would be convened to begin conducting assessments and providing information to the PEOC science section.
Public Communications: If not already done, communication teams will begin developing communication strategies to assist in coordinating messages with other communication teams. The province would begin disseminating geo-targeted emergency bulletins to notify the public of an event at the Pickering NGS and to instruct them to monitor media for possible protective actions they may need to take.
-
Notice of Anticipated Release but no order to take KI pills
There are two types of releases: a controlled filtered release, and an uncontrolled release. For a controlled filtered release, the radioiodine will likely be filtered from the release in which the ingestion of KI pills would not be required. In the very unlikely event of an uncontrolled release, there may be radioiodine in the release, which depending on the plume may require the ingestion of KI pills for specific keyholes within the IPZ.
In any case, plant conditions and meteorological data are used to determine well in advance when a release may occur, allowing for time to inform and implement protective actions. Specifically, stakeholders including the province, OPG, the CNSC and Health Canada would conduct independent assessments, and dispersion and dose modelling. OPG Response: OPG ERO would monitor plant conditions and provide information to the province, the CNSC, and other relevant stakeholders. If a controlled filtered release were anticipated, OPG would work with the province to determine venting strategies, e.g. timing of release to coincide with favourable meteorological conditions.
Provincial/Municipal Response: Throughout a response, the province would continue to provide updates and information to relevant stakeholders including MOH and municipal CEMCs. Many factors based on the event progression would be considered to prioritize and implement protective actions.
Logistical arrangements for distributing KI pills to areas of the IPZ:
Logistical and planning considerations for distributing KI to the IPZ would be discussed between OFMEM and the MOH, and other relevant stakeholders regardless of whether there has been an order to take KI pills. Items to discuss include:
- Logistical arrangements by the province to prepare the KI pills for delivery from the central facility.
- MOH to inform the CMOH that logistical requirements are being arranged for the distribution of KI pills to certain areas of the IPZ.
- The province will consider meteorological data and the timings of the anticipated release to determine where KI needs to be distributed within the IPZ. Based on planning and modelling, it is expected that distribution of KI pills to the entire IPZ would not occur.
- The province and MOH to liaise with the identified municipalities to make arrangements for the pre-staging of KI pills at municipal facilities.
The municipal CEMCs/PHUs would have received information from MOH and OFMEM on arrangements for pre-staging KI pills. The following information would be communicated to the municipalities: which municipalities will receive KI pills and whether there has been an order to take KI pills by the CMOH. The municipalities anticipating receiving pills will ensure that the logistical arrangements are in place at the appropriate facilities.
Under the direction of the CMOH and MOH, PHUs also have the jurisdiction to close schools and send students home if there was an anticipated release.
Public Communications: Each stakeholder would have activated their communication teams to respond to public inquiries, and disseminate information to the public through emergency bulletin boards. In all stages of the response, clear, consistent, and coordinated messaging is a priority for communicating with the public. Stakeholders are required to communicate information based on their jurisdiction, and continue to reinforce information disseminated by the province and OPG. A Joint Press Conference may also be considered with designated spokespersons from key stakeholders.
-
Notice of Anticipated Release, CMOH order to take KI pills
OPG Response: ERO maintaining situational awareness, and communicating and providing support to external stakeholders.
Provincial/Municipal Response: The order to take KI pills would be a recommendation from the PEOC Scientific Section to the CMOH. Ultimately, the CMOH has the authority in consultation with the PEOC, and the appropriate local Medical Officers of Health to order the ingestion of KI pills.
The province and the municipality CEMCs/PHUs will work together to ensure that KI pills are pre-staged in keyhole areas of the IPZ where the release is anticipated to travel. Additional distribution arrangements may be in place for facilities that require additional assistance due to larger vulnerable populations (e.g., long-term health care facilities).
Public Communications: Those in the IPZ who do not have KI pills will be provided with the required information on how to retrieve them from the pre-staged locations, and information for taking KI pills. KI Distribution in the DPZ would proceed in a similar manner as the IPZ, but would target the members of the public who lost, misplaced, or otherwise do not possess a pre-distributed supply. Extensive communication efforts will also be undertaken in the DPZ for communicating protective actions (evacuation strategies, sheltering in place), the release timings, and the time to ingest KI pills.
-
Release has ended. For the purposes of the exercise focused on the distribution of KI, the event has now ended and no further releases is anticipated.
Public Communications: Communications would focus on providing information that no further ingestion of KI pills is required. The information would be coordinated with all municipalities to ensure consistent messaging.
16. Additional items of discussion
-
CNSC Commission Update: CNSC indicated that an update of the KI Working Group would be presented at the CNSC Public Commission Meeting on November 6, 2019. CNSC showed participants how to tune into the live webcast of the meeting via the CNSC website.
-
Workshop feedback: Lessons learned and feedback for this workshop will be tracked via participant surveys that will be sent out to all participants following the workshop.
Action: CNSC to send out a questionnaire/feedback survey to workshop participants.
-
Indigenous Communities: Participants inquired about the correspondence between the Indigenous communities and the CNSC, and requested to be informed if there were any within their municipalities.
Action: CNSC to share the correspondence between the CNSC and the Indigenous Communities with Working Group members.
17. Path forward for draft report
The following actions have been identified to meet the deliverables set out for Phase I of the KI Pill Working Group:
- Action: CNSC to draft and share workshop Meeting Minutes to all Working Group members by November 19, 2019.
- Action: CNSC to propose teleconference dates with all Working Group members to discuss the workshop Meeting Minutes by November 19, 2019.
- Action: Working Group members to provide comments on the workshop Meeting Minutes by December 3, 2019.
- Action: CNSC to French translate the workshop Meeting Minutes and post to the CNSC website.
- Action: CNSC to draft the Phase I report for review by Working Group Members by December 2019.
- Action: Working Group members to review the Phase I report and provide concurrence on the information presented (Date TBD).
- Action: Signatories of the Working Group to approve the Phase I report (Date TBD).
- Action: Phase I report to go through public comment period (Date TBD).
18. Closing Remarks
The Signatory Representatives thanked all the participants for their participation in the KI Pill Working Group Phase I Workshop and their ongoing support to the overall KI Pill Working Group.
The workshop provided an opportunity for stakeholders involved in a nuclear emergency response to build stronger working relationships and coordinate efforts to enhance emergency preparedness and response. Reoccurring themes were noted throughout the workshop, this included the importance of public awareness and communications strategies, and leveraging existing resources to support all-hazards events.
Overall, the workshop was successful in engaging participants and maintaining focussed discussions to work towards meeting the deliverables set out for Phase I of the Working Group.
Workshop Day 2 ended at 15:30 on Tuesday November 5, 2019.
Page details
- Date modified: